
ALL MATERIAL COPYRIGHT KEVIN SCOTT 2011. LINKS TO THIS SITE ARE WELCOME BUT DO NOT COPY MATERIAL FROM THIS SITE TO ANY OTHER WEBPAGE.



If you find this site useful, please support it by making a donation of $1 to help maintain and develop it. Click on the PAYPAL DONATE button to do this safely. But there is no obligation - please avail yourself of the information and facilities of the site at no charge.
This article is about the measurement and relief of dental pain. It is not a report of a survey of dental pain, nor can it be remotely said to be a "study" of the subject.The author is not a medical practitioner but a scientist and this report is of a single experiment carried out when he, the author was suffering dental pain and waiting for treatment. Suffering from an abscess under a lower left molar, he was prescribed Naproxen by a physician. Naproxen is an anti-inflammatory and proved very effective against toothache. Aspirin and codeine were not very effective, with limited or no anti-inflammatory properties. Ibuprofen, although an anti-inflammatory was also not very effective at pain relief in this case.
Naproxen has two main advantages in its use for dental pain relief: (a) It is a powerful anti-inflammatory which is exactly what is required for toothache relief. Toothache is very painful because any inflammation is constrained under the tooth and has no space in which to expand. Therefore the pressure the inflammation exerts is very high and the pain correspondingly great. An anti-inflammatory is thus the best option for effective relief. ( Alongside antibiotics)
Pharmacokinetics
(b) The second advantage of naproxen is its long pharmacological elimination half-life.It is rapidly absorbed in the gastro-intestinal tract and reaches a peak concentration in blood plasma 1-2 hours after administration. The decay of concentration follows approximately first-order kinetics with a half-life of about 15 hours. Thus the rate constant for the first order decay is 0.046hrs-1. The kinetics are more complicated than this simple treatment suggests and are affected by other drugs and metabolites present in the blood-stream. As a guide to dosage and the effectiveness of pain relief, however, this simple picture is of some use.
Dental Pain
The estimation and quantification of pain is difficult. The author found that with toothache, several levels are discernible. At its lowest level (Level 1) toothache is not continuous, only experienced when eating or chewing on one side, or when very hot or cold foods enter the mouth. Level 2 is a dull continuous ache which is minimal when there is no oral activity (eating or speaking), but increases with speech or chewing. Level 3 is increased pain, but at such a level that thinking and working, although less efficient are not inhibited altogether. Level 4 is reached when the pain is so intense that it and efforts to relieve it form the whole agenda of the patient. Level 5 is desperation!
The plots
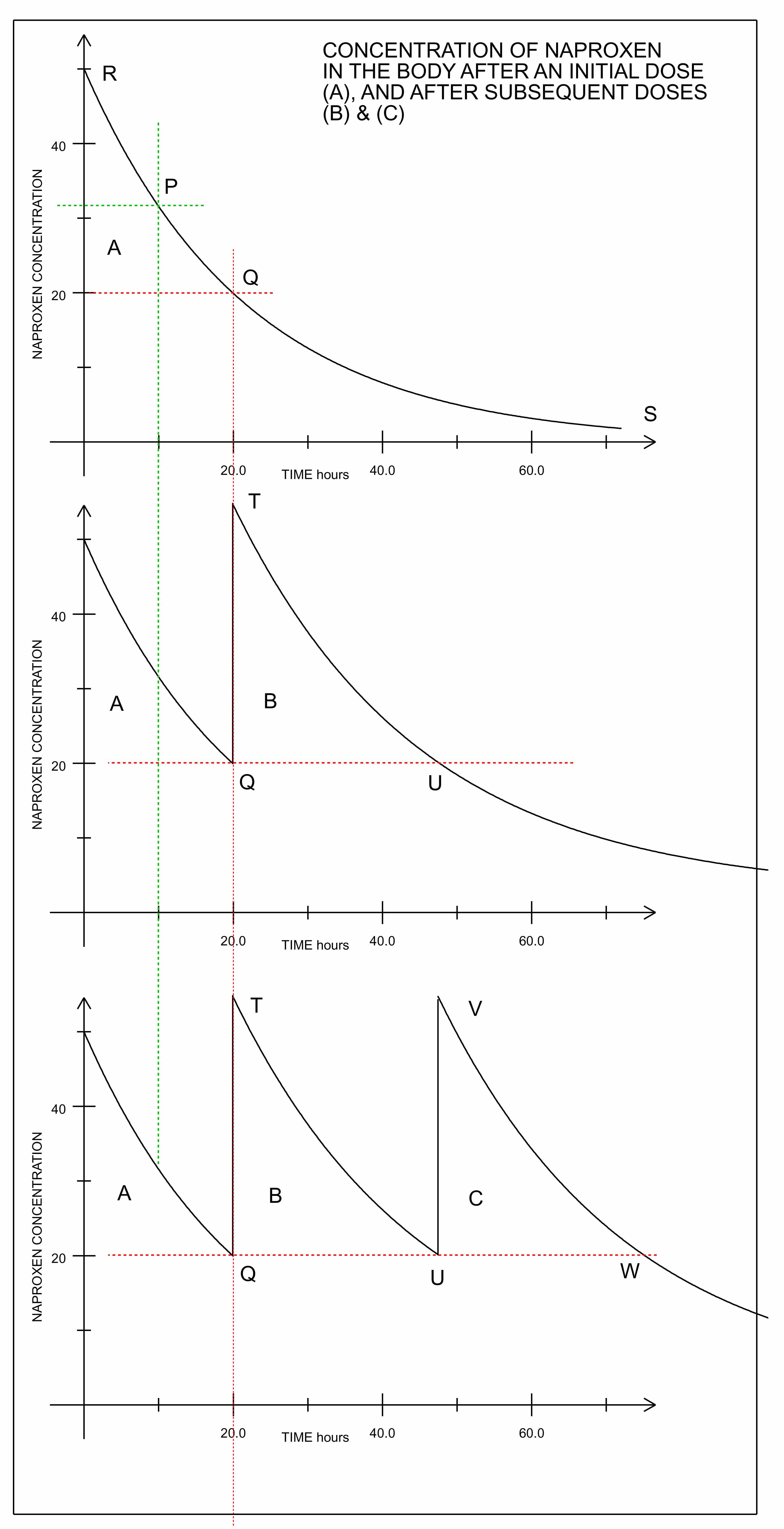
The top plot shows the calculated amount of Naproxen remaining in the blood serum with time from the ingestion of a single dose. The Naproxen level falls exponentially with time. It was found by the author that the initial dose completely quenched the toothache (at level 4) and that for some hours it was entirely absent. Then, it reappeared fairly sharply. In one instance it reappeared after 10 hours when the Naproxen level had fallen to point P on the top plot. The Naproxen level corresponding to that point represents the minimum required level which will just quench the pain at its current level. To obtain this number by experiment is useful as it gives something of a quantitative reading of the intensity of the dental pain. If is a subsequent experiment, the pain reappears at point Q in the top plot, this gives a revised estimate of the current pain intensity. It is clear that these kinds of experiments can be used to give a measure of the pain level and to determine whether is it getting worse or better.
Subsequent Naproxen doses
The middle and lower plots show the effect of repeated dose upon the Naproxen level. If the pain reappears at point Q, it is only necessary to raise the Naproxen level just above that at Q, to relieve it. In principle, this could be done with the successive administration of a series of small doses, to keep the Naproxen level just above Q. In practice, a single 250 mg tablet is taken which raises the Naproxen level to T. This then declines over a period of hours to U. If the pain level does not alter, the point U can be predicted in hours from the second dose, whereupon, when it does break through, it can be relieved by a third dose of a single Naproxen tablet. If the pain breaks though earlier, it can be concluded that it is becoming more intense, and if later, that it is becoming more moderate.
The Dose
One of the advantages of this semi-quantitative approach to Naproxen usage, is that it can minimise the dose to that which is strictly necessary. If the pain level corresponds to point Q, then any Naproxen level above Q is redundant. As there are undesirable side-effects of Naproxen, clearly it is an advantage to maintain the dose only marginally above that required to relieve the pain completely. Thus after the initial 2 tablet dose (500 mg) only a single pill of 250 mg is taken on subsequent doses.